Women are more vulnerable to many sided health hazards of alcohol. According to the WHO status report on health and alcohol, “there is evidence that women may be more vulnerable to alcohol-related harm from a given level of alcohol use or a particular drinking pattern.
omen are more vulnerable to many sided health hazards of alcohol. According to the WHO status report on health and alcohol, “there is evidence that women may be more vulnerable to alcohol-related harm from a given level of alcohol use or a particular drinking pattern. The vulnerability of females to alcohol-related harm is a major public health concern because alcohol use among women has been increasing steadily in line with economic development and changing gender roles and because it can have severe health and social consequences for newborns….
However, for health outcomes such as cancers, gastrointestinal diseases or cardiovascular diseases, the same level of consumption leads to more pronounced outcomes for women.” The vulnerability of women may be explained by a wide range of factors. For example, women typically have lower body weight, smaller liver capacity to metabolize alcohol, and a higher proportion of body fat, which together contribute to their achieving higher blood alcohol concentrations than men for the same amount of alcohol intake. Women are also affected by interpersonal violence and risky sexual behaviour as a result of the drinking problems and drinking behaviour of male partners. Moreover, alcohol use has been shown to be a risk factor for breast cancer.
Also many societies hold more negative attitudes towards women’s drinking alcohol than men’s drinking, and especially towards their harmful drinking, which, depending on the cultural context, may increase women’s vulnerability to social harm. Finally, women who drink during pregnancy may increase the risk of fetal alcohol spectrum disorder (FASD), and other preventable health conditions in their new-borns. In some cultures women have been protected from alcohol consumption by strong traditional values. For example, in the WHO region which includes India and nearby countries only 5 per cent of women consume alcohol whereas in the WHO region where the USA and nearby areas are included, more than 50 per cent of women consume alcohol. Imagine the public health and social disaster that could result if alcohol consumption by women in India reaches the level of the USA. Yet, promoting alcohol consumption among women as a sign and symbol of liberating modern trends is widely practiced in India. According to the WHO, alcohol consumption in adolescents, especially binge drinking, negatively affects school performance, increasing participation in crime and leads to risky sexual behaviour. The WHO quotes growing scientific evidence that has demonstrated the special harmful effects of alcohol consumption prior to adulthood on brain; mental; cognitive and social functioning of youth and increased likelihood of adult alcohol dependence and alcohol related problems among those who drink before physiological maturity. The WRVH says especially in the context of youth violence that drunkenness is an important immediate situational factor that can precipitate violence. In a Swedish study on youth-violence, about three-quarters of violent offenders and around half the victims of violence were intoxicated at the time of the incident. Several surveys indicate high end rapidly increased consumption of alcohol amongst youth. What is particularly worrying is high consumption at a very tender age which is likely to be very harmful for the brain and also lead to much higher risk of alcohol dependence in later years.
For example, in the UK, binge drinking thrice or more a month is reported among 33 per cent of adolescents in the 15-16 age groups. Binge drinking levels affecting between 25 to 40 per cent of youth are quite common now. Among elderly people the possibility of alcohol reaching and affecting sensitive organs including brain, liver and muscles is higher compared to younger people. The WRVH report says that reducing the availability of liquor can be an important community strategy to reduce crime and violence as research has shown alcohol to be an important situational factor that can precipitate violence. In a 4-year study conducted in New Zealand, crime rates in situations of high and low availability of alcohol were compared.
This study revealed that crime rates fell significantly for two years in areas of reduced alcohol availability. According to a report prepared by the National Council on Alcoholism and Drug Dependence, USA (NCADD), alcohol and drugs are implicated in an estimated 80 per cent of offences leading to incarceration in the USA such as domestic violence, driving while intoxicated, property offences, drug offences and public order offences. Alcohol is a factor in 40 per cent of all violent crimes and according to the Department of Justice, 37 per cent of about 2 million convicted offenders currently in jail report that they were drinking at the time of the event. Alcohol, more than any illegal drug, was found to be closely associated with violent crimes including murder, rape, assault, child and spousal abuse.
About 3 million violent crimes occurred each year in the USA in which victims perceived the offenders to have been drinking and statistics related to alcohol use by violent offenders show that about half of all homicides and assaults are committed when the offender, victim or both have been drinking. This report by NCADD points out that alcohol is often a factor in violence where the attacker and the victim know each other. Two thirds of victims who were attacked by an intimate (including a current or former spouse, boyfriend or girlfriend) reported that alcohol had been involved. More than 1 million are arrested for driving while intoxicated in a year in the USA. Drinking and drugged driving is the number one cause of death, injury and disability of young people under the age of 21.
Keeping in view all health and social impacts it is clear that the high levels of consumption of alcohol and various intoxicants is very harmful. In developing countries like India as well in some of the poorest countries and regions, millions of families are being devastated economically too because of the consumption of alcohol and intoxicants, both in terms of the money they pay for intoxicants and also in terms of the ruin of health. The various stages of the cycle of manufacture, sale and consumption of various intoxicants also involves very heavy ecological costs. Hence there is a very strong case for public campaigns being carried out with continuity and sincerity in rural as well in urban areas to reduce the consumption of alcohol and other intoxicants as much as possible
Bharat Dogra
Source: The Statesman, 16/03/24
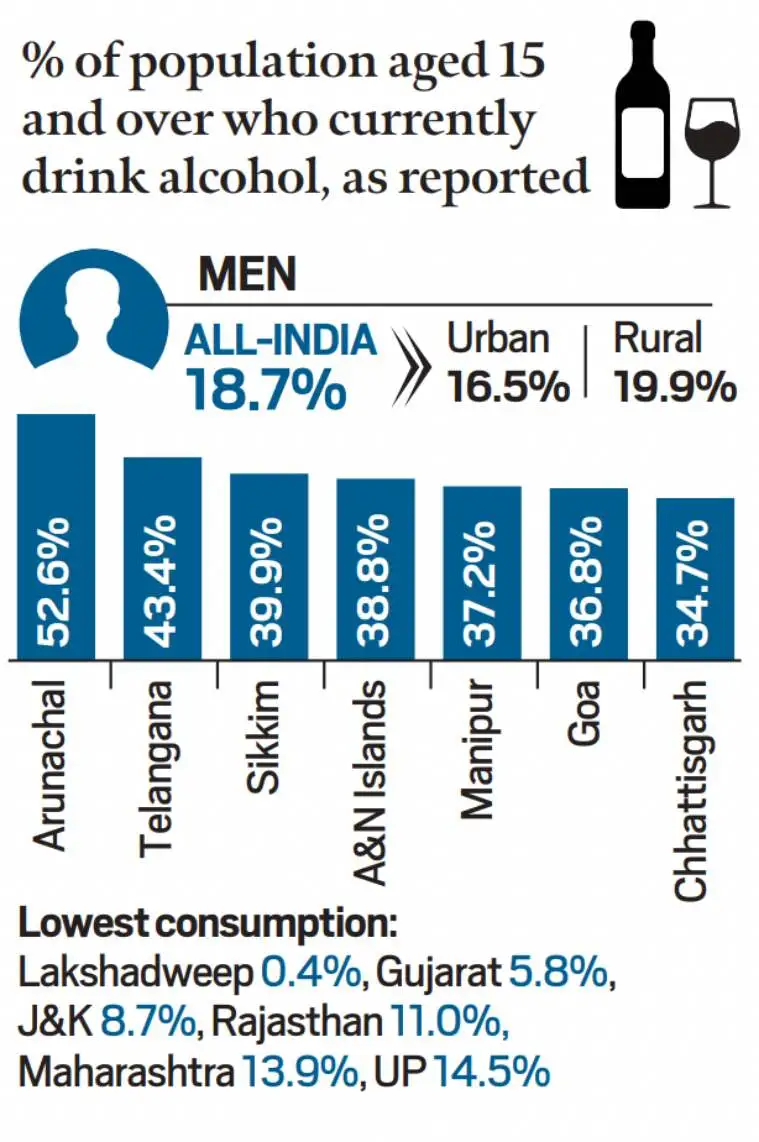 Source: NFHS-5
Source: NFHS-5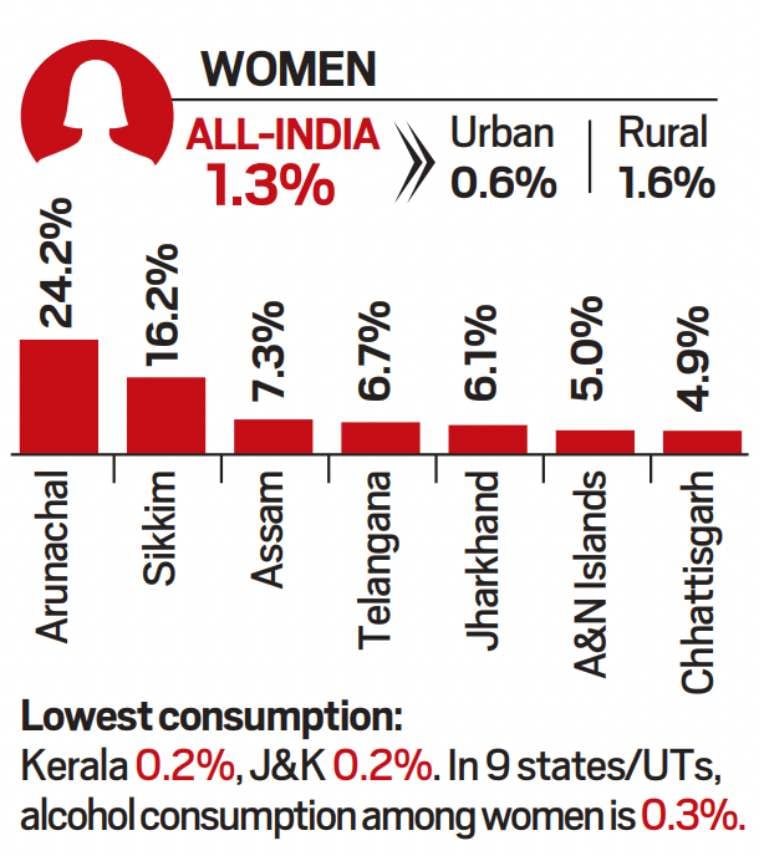 Source: NFHS-5
Source: NFHS-5
 The data comes at a time when India is on the verge of implementing stricter tobacco control laws. From April 1, 2016, the Indian government will be implementing ‘plain packaging’ as directed by the Allahabad High Court, following a writ petition on the matter.
The data comes at a time when India is on the verge of implementing stricter tobacco control laws. From April 1, 2016, the Indian government will be implementing ‘plain packaging’ as directed by the Allahabad High Court, following a writ petition on the matter. India became a party to the WHO Framework Convention on Tobacco Control (FCTC) on February 27, 2005. Since then India has implemented a series of measures leading to the current status of increased social awareness. Soon after signing the WHO FCTC, smoking was completely banned in many public places and workplaces in India — with the new law permitting establishments to create smoking zones within restaurants, airports and hotels having 30 or more rooms.
India became a party to the WHO Framework Convention on Tobacco Control (FCTC) on February 27, 2005. Since then India has implemented a series of measures leading to the current status of increased social awareness. Soon after signing the WHO FCTC, smoking was completely banned in many public places and workplaces in India — with the new law permitting establishments to create smoking zones within restaurants, airports and hotels having 30 or more rooms. It is a “unique” tobacco product due to its availability in myriad varieties, easy access, and affordability, especially for adolescents. It has been studied to be a “gateway product and facilitates initiation,” writes Dr. Monica Arora in a 2012 paper on consumption of SLT in India.
It is a “unique” tobacco product due to its availability in myriad varieties, easy access, and affordability, especially for adolescents. It has been studied to be a “gateway product and facilitates initiation,” writes Dr. Monica Arora in a 2012 paper on consumption of SLT in India.



